Topol named the longitudinal-data wedge.
TL;DR [show]
Eric Topol's NYT-bestseller 'Super Agers' (2025-05-06) argued multimodal AI integrating omics, lifestyle, and clinical data can predict cardiovascular, cancer, and neurodegenerative disease decades in advance — and that GLP-1s are a structural shift, not a fad. Operator read: the longitudinal-data wedge is the actual operator playing field; the prevention-vs-treatment economic question rides on whose data graph compounds, and Topol names the candidates without naming the moat.
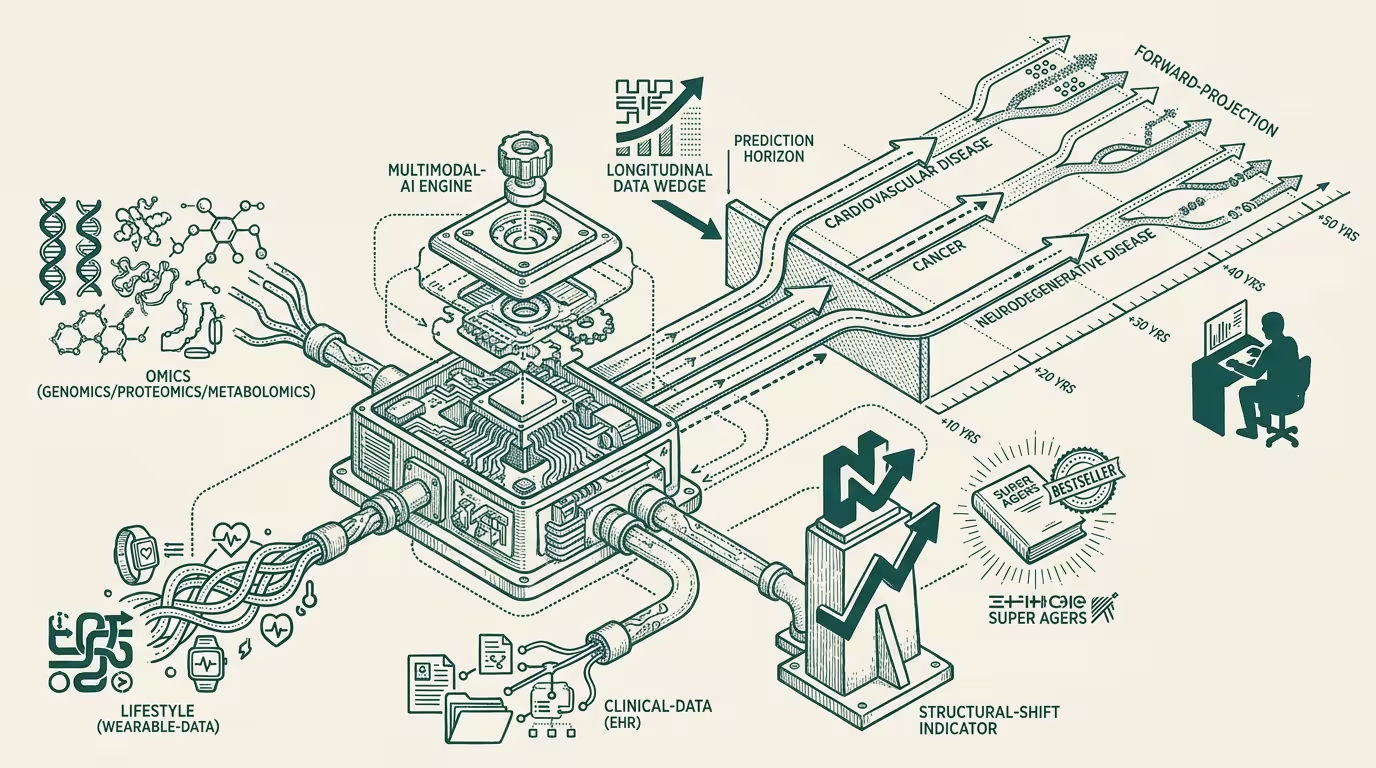
Eric Topol published "Super Agers" on May 6, 2025. The book hit the NYT bestseller list within two weeks and became the canonical 2025 reference for the longitudinal-data thesis in healthcare-AI. The load-bearing argument: multimodal AI integrating omics (genomics, proteomics, metabolomics), lifestyle data (wearables-class continuous biometric capture), and clinical data (EHR, imaging, lab values) can predict cardiovascular, cancer, and neurodegenerative disease decades in advance. The book reads as a clinical-class engagement with the prevention-vs-treatment economic shift that the GLP-1 era made operationally visible.
The trade press read it as a prevention-medicine vision document. The part that holds is sharper.
Topol named the longitudinal-data wedge — the operating playing field where the prevention-vs-treatment economic question is actually decided — and the book is, in operating terms, the first widely-read articulation of the structural opportunity. _The prevention-vs-treatment economic question rides on whose data graph compounds._ Topol names the candidates without naming the moat.
Compare point-in-time data with longitudinal data and the structural argument surfaces. A point-in-time clinical encounter captures the patient's state at a single moment. The encounter generates a record. The record sits in the EHR. The record's predictive value is bounded by the snapshot it captured. A longitudinal-data graph that captures continuous biometric data, periodic clinical encounters, and episodic genomic-and-omics measurements over ten-plus years produces a per-patient predictive signal that no point-in-time data captures. The signal supports decade-ahead disease prediction at clinical-actionable confidence levels. The signal also supports patient-specific prevention-program calibration that no generic prevention guideline matches.
The moat is the data graph itself, not the AI capability operating on it. Topol names this directionally without specifying the operator-class implication: whichever operator owns the data graph at scale captures the prevention-economy rents in a category that, by 2035, looks structurally larger than the current treatment economy.
The candidates Topol names cover the surface. Apple's Health platform plus Apple Watch (consumer-side, lifestyle-data dominant). Oura, Whoop, Fitbit (consumer-side wearables, narrower data envelope). 23andMe and Color (genomic, episodic). The Function Health and Forward Health class (subscription-class clinical-data capture). Verily and Iora-class (provider-integrated longitudinal data). Each candidate has a data-graph fragment. None of the candidates, in 2025, owns a complete longitudinal-data graph at scale.
Trace it back to the strategic playing field for healthcare-AI capital allocation in 2025-2030 and the wedge sharpens. Operators investing in healthcare-AI without a position on the longitudinal-data wedge are investing in capability that will be commoditized as the longitudinal-data-graph operators capture the prevention-economy. The capital-allocation question is not "which AI capability" but "which data-graph operator." The investment thesis that doesn't specify a data-graph position is operating-thin against the thesis that does.
Trace it back to the GLP-1 evidence and the prevention-economy shift surfaces. Topol's framing of GLP-1s as a structural shift rather than a fad is correct. The GLP-1 class is the first prevention-economy intervention to demonstrate scale-class economic impact. The class produced market-cap shifts in the pharma industry visible at the public-company-equity layer, not just at the trade-press-coverage layer. The structural read is that prevention-economy interventions are now investor-class-bankable. Other prevention interventions calibrated to longitudinal-data-graph signals will follow the same structural arc through 2027-2030.
Trace it back to the moat-mechanism analysis and the data-collection layer surfaces. The moat is the data-collection mechanism, not the data itself. A longitudinal-data graph is durable in proportion to the operator's ability to keep collecting data over decades. The mechanism includes consumer engagement (continuous-wearable retention rates), clinical-integration (provider-network breadth), payer-relationship depth (reimbursement support for longitudinal-data programs), and regulatory positioning (HIPAA-compliance, the patient-data-portability rules that govern data exit). Each is an operator-tier moat layer. Operators with mechanism depth in all four layers are operator candidates for capturing the longitudinal-data-graph economy. Operators with only one or two layers are partial candidates whose moat depth is fragile.
The same shape recurs across categories beyond cardiovascular, cancer, and neurodegenerative disease. Mental-health prevention has its own longitudinal-data signal. Metabolic-health prevention has its own. Reproductive-health and aging-economy interventions each have their own. Each category has its own operator-tier candidate set and its own moat-mechanism specifics. Topol's framing applies to the cardiovascular-cancer-neurodegenerative trifecta cleanly; the framing extends to adjacent categories with category-specific calibration.
What survives all of this is that "Super Agers" is one of the cleaner clinical-class articulations of the longitudinal-data wedge in 2025, the moat-naming gap is the operator signal the book is silent on, and the operator-tier discipline is to translate Topol's candidates into specific data-graph-mechanism positions and to invest against those positions explicitly. Operators who do that work in 2025-2026 are positioned for the prevention-economy shift through the late 2020s. Operators who treat the book as vision-class reading without translating to operating-class positions are missing the structural opportunity the book is, in operating practice, naming.
Topol named the longitudinal-data wedge. The candidates are visible. The moat is the data-collection mechanism that compounds across decades. The operator question is which of the candidates has the mechanism depth to capture the prevention-economy rents the wedge creates. Most analyses of the candidates do not run the mechanism-depth analysis. The ones that do are the analyses operating against the actual operator-level playing field.
—TJ